Ileoileal Intussusception Due To Meckel’s Diverticulum - An Uncommon Etiology
Intussusception is a major cause of acute intestinal obstruction in children. Here is an unusual case of ileoileal intussusception due to inverted Meckel’s diverticulum in a baby.
Author:Suleman ShahReviewer:Han JuSep 21, 202454.5K Shares727.5K Views
We are presenting ileoileal intussusception due to Meckel’s diverticuluminvolving a male baby.
Most cases of intussusception (90%) are considered idiopathic in origin, as they are not associated with any lead point pathology. Only about 6% of cases have been found to be associated with a pathological defect, which is primarily a Meckel’s diverticulum.
Meckel’s diverticulum is the most common congenital abnormality of gastrointestinal tract occurring in 1% to 2% of the population and represents an incomplete involution of the omphalomesenteric duct.
It is usually asymptomatic throughout lifeand clinically present only when complications arise. Intestinal obstruction due to Meckel’s diverticulum is the second most common presentation in children.
Preliminary Discussion
Various mechanisms causing intestinal obstruction in association with Meckel’s diverticulum are:
- volvulus of the small intestine around congenital omphalomesenteric and mesodiverticular bands
- intussusception
- due to incarceration within a hernia sac (Littre hernia)
- stricture secondary to chronic diverticulitis
- foreign body
- lithiasis of Meckel's diverticulum
- neoplasm
The incidence of intussusception due to Meckel’s diverticulum accounts for only 4% of all cases of intussusceptions and it is mostly seen in children of >2 years of age and adults.
It occurs due to inversion of Meckel’s diverticulum into the bowel lumen, which serves as a lead point lesion for ileoileal or ileocolic intussusception.
This paper reports a case of an uncommon etiology of ileoileal intussusception due to Meckel’s diverticulum.
Case Report
An 18-month-old male baby was taken to the emergency department of our institution, with a historyof:
- on and off colicky pain in the abdomen
- blood in stools for the past 24 hours
Episodes of pain used to last for a few minutes and were occasionally associated with vomiting.
The child was being treated conservatively at home and he was refusing any feed for the same duration. He had developed abdominal distention in the last 6 hours and became listless.
There was no history of:
- respiratory infection
- diarrhea
- trauma
On examination, the child was lethargic and dehydrated, with a:
- heart rate of 128 beats/minute
- blood pressure of 80/60 millimeters of mercury (mmHg)
He presented gross distension with profound tenderness all over the abdomen suggestive of peritonitis. Owing to distension, no mass or organomegalywas palpable.
There was polymorphonuclear leukocytosis on hematological investigations, but other parameters were normal.
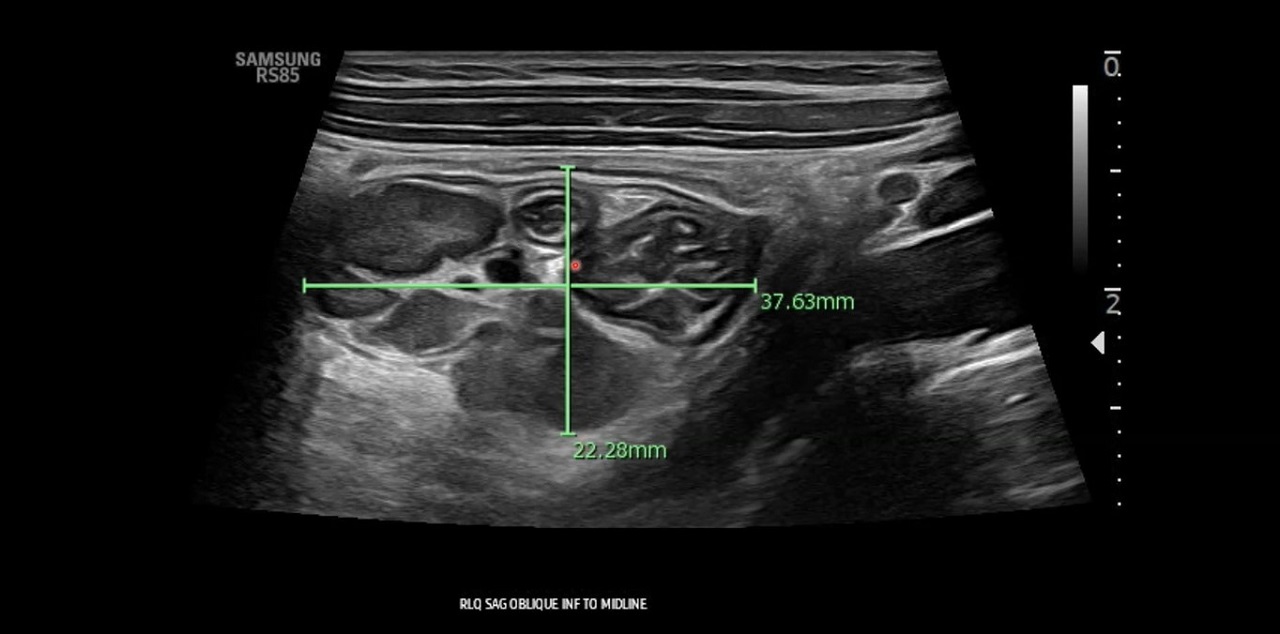
Plain X-ray of the abdomen revealed free gas in the peritoneal cavity, with multiple air fluid levels. Abdominal sonography confirmed these findings and additionally suggested the possibility of intussusception.
After resuscitation, the child was taken for emergency laparotomy.
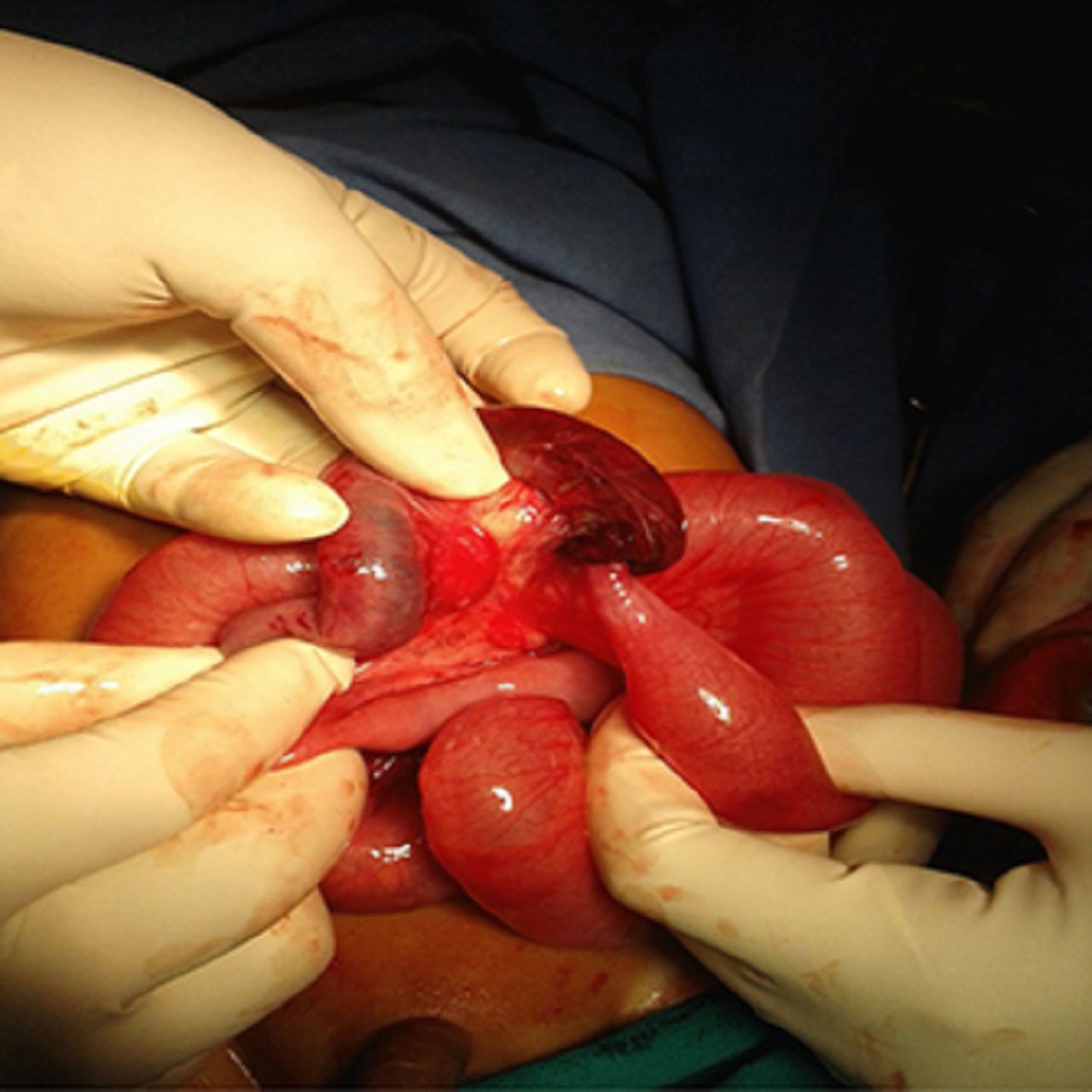
During surgery, on opening the abdomen, there was a large amount of hemorrhagic fluid in the peritoneal cavity with a gangrenous ileoileal intussusception.
This intussusception was approximately 5 centimeters of ileum invaginating into the distal segment of the ileum, approximately 25 centimeters from the ileocolic junction (see picture below). The picture shows ileoileal intussusception with gangrene.
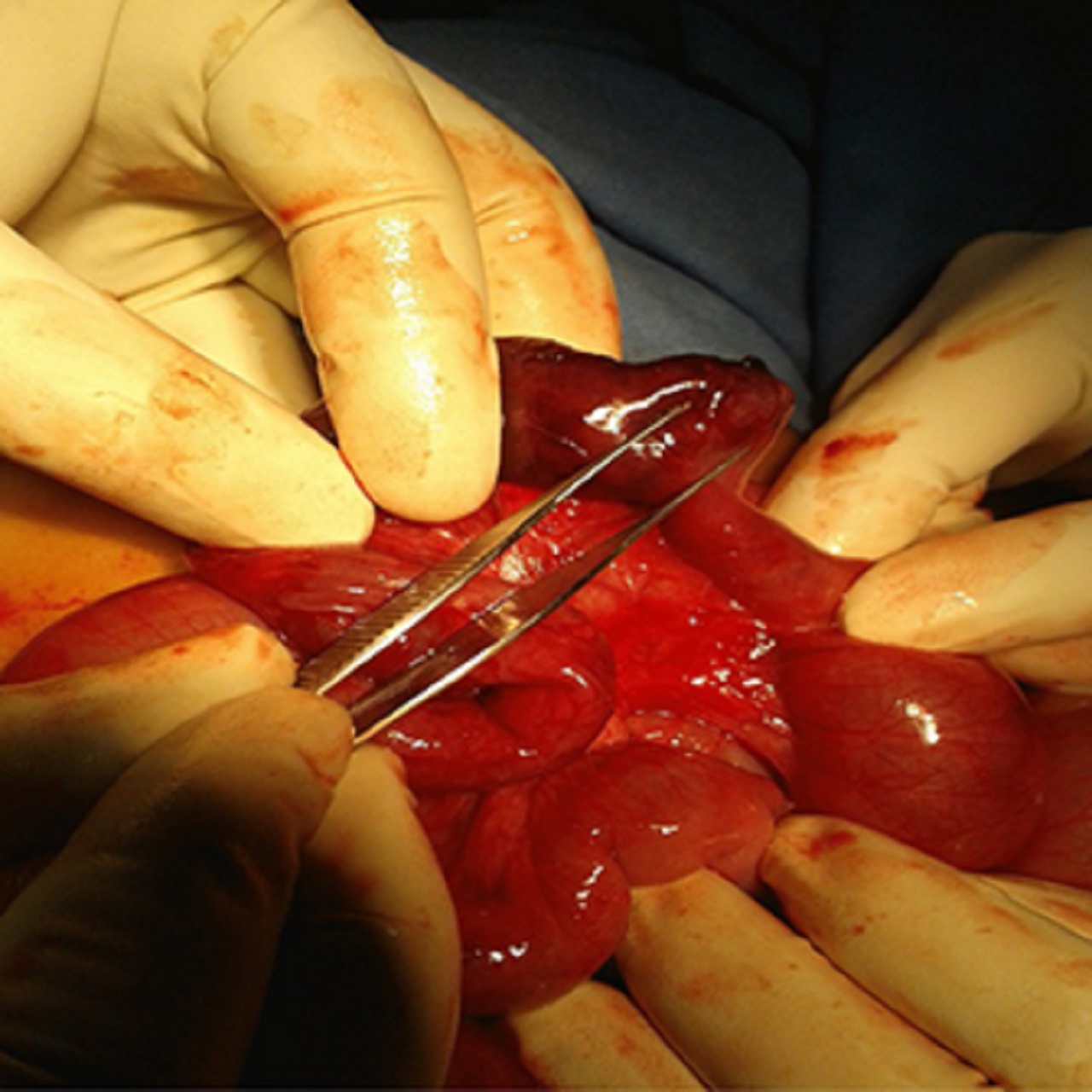
On reduction, we found a Meckel’s diverticulum at approximately 30 centimeters from the IC junction (ileocaecal junction or ICJ), acting as a lead point lesion for this intussusception (see picture below).
Whole intussuscepted segment of the ileum was gangrenous, so the gangrenous bowel was resected and continuity was restored by ileoileal anastomosis.
Oral intake of food was started on the third post-operative day. The rest of the post-operative period was uneventful, and the child was discharged on the eighth post-operative day.
Main Discussion
Intussusception is one of the most frequent causes of bowel obstruction in the pediatric population, with a reported incidence of 1.5 to 4 cases per 1,000 live births.
Intussusception is usually seen in children aged between 3 months and 3 years and 80% of them occur before the age of 2 years. The majority of the pediatric cases (95%) are of ileocolic type and Meckel’s diverticulum is considered a rare cause.
The classic clinical triad of intussusception is colicky abdominal pain, vomiting and bloody (red currant jelly) stools; however, it is found in only 20% of patients.
In ileocolic type, abdominal examination may reveal a sausage-shaped mass in the right upper quadrant along with empty right iliac fossa.
Clinical presentation in pediatric intussusception may range from:
- painless intussusception to constipation
- vomiting
- dehydration
- diarrhea
- intestinal prolapse
- sepsis
- shock
- syncope
- altered mental status (lethargy or irritability)
Intussusception is likely to be fatal in 2 to 5 days, of onset of symptoms, if left untreated.
Plain X-ray of the abdomen is usually the first investigation done in cases of suspected intestinal obstruction. However, its sensitivity is only 45% for the diagnosis of intussusception.
Classic plain radiograph findings for intussusceptions are absence of air in the ascending colon, a soft tissue density in the upper abdomen, target sign or crescent sign.
Abdominal sonography is a fast non-invasive test with high sensitivity (98 to100%) and specificity (88 to 100%) if performed by skilled personnel.
Classical findings on sonography include the:
- target lesion or doughnut sign on transverse view
- pseudokidney sign on longitudinal view
Although considered the investigation of choice in adults (sensitivity and specificity in the range of 88 to 100%), computed tomography is usually not indicated in children due to radiation exposure and sedation-associated risk.
Air, water-soluble, or barium contrast enemas are diagnostic approaches with significant therapeutic value, with reduction rate between 70% and 90%.
At present, air contrast enema is considered as the gold standard for pediatric intussusceptions, as barium enema has a risk of perforation with chemical peritonitis and shock.
Barium enema is contraindicated in suspected bowel ischemia with:
- necrosis
- severe shock
- sepsis
- extreme age
Surgical intervention is indicated if intussusception is not reduced by an enema or if the following features are evident:
- bowel ischemia
- perforation
- shock
- peritonitis
You Might Like: Playing The Long Game: Strategies For A Healthy Lifestyle
Conclusion
The diverticulum was named after Johann Friedrich Meckel, the Younger (1781-1833), a renowned German anatomist and a professor of anatomy, pathology, and zoology.
Meckel’s diverticulum may act as a lead point lesion for childhood intussusceptions. Delay in seeking medical advice or delay in diagnosis may lead to ischemic necrosis and perforation of the involved bowel.
More studies regarding ileoileal intussusception due to Meckel’s diverticulum should be made.

Suleman Shah
Author
Suleman Shah is a researcher and freelance writer. As a researcher, he has worked with MNS University of Agriculture, Multan (Pakistan) and Texas A & M University (USA). He regularly writes science articles and blogs for science news website immersse.com and open access publishers OA Publishing London and Scientific Times. He loves to keep himself updated on scientific developments and convert these developments into everyday language to update the readers about the developments in the scientific era. His primary research focus is Plant sciences, and he contributed to this field by publishing his research in scientific journals and presenting his work at many Conferences.
Shah graduated from the University of Agriculture Faisalabad (Pakistan) and started his professional carrier with Jaffer Agro Services and later with the Agriculture Department of the Government of Pakistan. His research interest compelled and attracted him to proceed with his carrier in Plant sciences research. So, he started his Ph.D. in Soil Science at MNS University of Agriculture Multan (Pakistan). Later, he started working as a visiting scholar with Texas A&M University (USA).
Shah’s experience with big Open Excess publishers like Springers, Frontiers, MDPI, etc., testified to his belief in Open Access as a barrier-removing mechanism between researchers and the readers of their research. Shah believes that Open Access is revolutionizing the publication process and benefitting research in all fields.

Han Ju
Reviewer
Hello! I'm Han Ju, the heart behind World Wide Journals. My life is a unique tapestry woven from the threads of news, spirituality, and science, enriched by melodies from my guitar. Raised amidst tales of the ancient and the arcane, I developed a keen eye for the stories that truly matter. Through my work, I seek to bridge the seen with the unseen, marrying the rigor of science with the depth of spirituality.
Each article at World Wide Journals is a piece of this ongoing quest, blending analysis with personal reflection. Whether exploring quantum frontiers or strumming chords under the stars, my aim is to inspire and provoke thought, inviting you into a world where every discovery is a note in the grand symphony of existence.
Welcome aboard this journey of insight and exploration, where curiosity leads and music guides.
Latest Articles
Popular Articles