Autonomic Dysreflexia Spinal Cord Injury - What Is It? Causes, Symptoms And Treatment
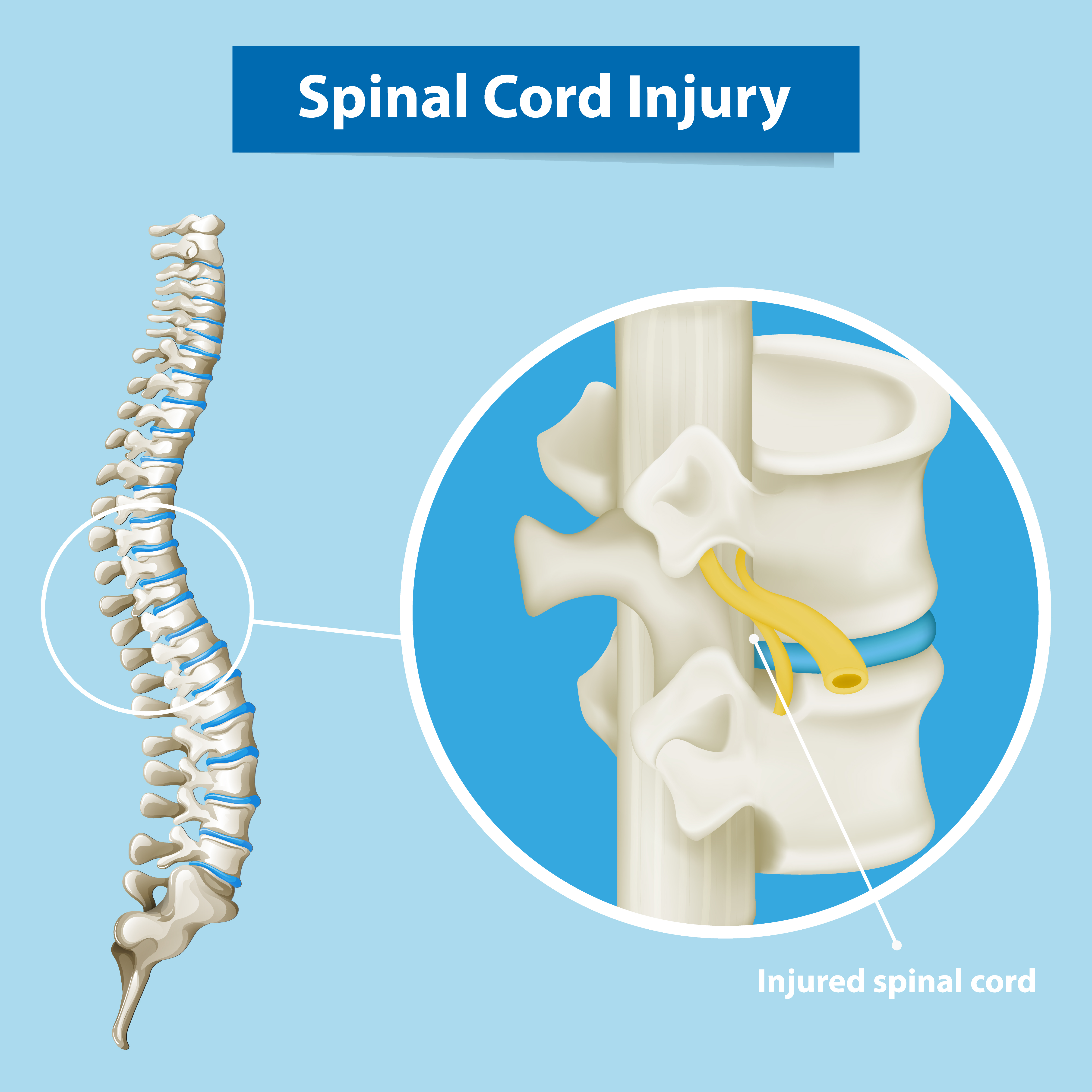
Autonomic dysreflexia spinal cord injury is a disorder that develops after a spinal cord injury, generally above the sixth thoracic vertebral level (T6). Up to 90% of patients with cervical or high-thoracic spinal cord injuries are at risk; the risk rises with the severity of the injury.
Author:Suleman ShahReviewer:Han JuSep 29, 2022241.9K Shares3.5M Views
Autonomic dysreflexia spinal cord injuryis a disorder that develops after a spinal cord injury, generally above the sixth thoracic vertebral level (T6). Up to 90% of patients with cervical or high-thoracic spinal cord injuries are at risk; the risk rises with the severity of the injury.
Autonomic dysreflexia is a potentially life-threatening clinical disease characterized by episodes of severe, uncontrolled hypertension. Everyone who works with people who have had spinal cord injuries should be familiar with this condition, its symptoms, its causes, and its treatment strategy.
What Is Autonomic Dysreflexia Spinal Cord Injury?
Spinal cord injuries often cause autonomic dysreflexia, which can be fatal if left untreated. It has a mortality rate of 22% and raises the risk of stroke by 300% to 400%.
Clinicians working in emergency or urgent care may not meet patients with this illness frequently, but when they do, fast diagnosis and treatment are necessary. This helpful reference provides a high-level explanation of autonomic dysreflexia and its diagnostic criteria.
For those with a spinal cord injury above the T6 level, autonomic dysreflexia manifests as an incoherent response to noxious stimuli below the degree of damage. It is three times more common in those who have had a full spinal cord injury (91%) than in those who have sustained only partial damage (27%).
Acutely raised systolic blood pressure of 25 mm Hg or more over the patient's typical values constitutes a clinical diagnosis of autonomic dysreflexia.

Autonomic Dysreflexia Made Easy
Autonomic Dysreflexia Spinal Cord Injury Symptoms
Some of the symptoms of autonomic dysreflexia, which may manifest suddenly, include
- Severe Paroxysmal Hypertension coupled with throbbing Headaches
- Excessive perspiration and painfully erect piloerection
- Changes in skin color and temperature above the lesion (Vasodilatation)
- Bradycardia
- Below the area of damage, the skin is cool and pallid (vasoconstriction).
- Visual abnormalities, dizziness, and worry or a sensation of dread, which is occasionally accompanied by cognitive impairment.
Causes Of Autonomic Dysreflexia
Even minor irritations, such as a full bladder or an ingrown toenail, may set off a chain reaction of nerve reactions. Additionally, the following may trigger the condition:
- Constipation
- Urinary calculi
- Yeast infection in the urinary tract
- Putting a catheter, a tube used in medicine, in a patient
- Hemorrhoids
- Damaged skin prone to blistering
- Skin breakdown due to pressure
- Burns may be caused by direct sunlight or by immersion in hot water.
- Put the scrotum under some pressure
- Sexual stimulation
- Period pains
- Close-fitting garments
Autonomic Dysreflexia Treatment
Ask The Patient And Caregiver
Since most patients will have had prior episodes, it is acceptable to ask them what their most frequent triggering event is and what their customary cure is. If a patient has a historyof autonomic dysreflexia, they likely understand the issue and are willing to take action.
Patients who are at risk for autonomic dysreflexia should always have a pack or kit on hand with appropriate pharmacological treatments and an emergency card or summary of autonomic dysreflexia to explain the illness and its acute treatment to people who don't know about it in case of an emergency.
Immediate First Steps
In the case of an episode, sit the patient upright with their legs hanging and remove any tight garments or constrictive devices. This will assist in dropping their blood pressure orthostatically by pooling blood in the abdomen and lower extremity capillaries and removing any triggering factors.
Vital signs should be continuously examined and the cause should be identified quickly. Check your blood pressure every 5 minutes and consider an arterial line. Immediately remove unpleasant stimuli.
Bladder over-distension is the most common trigger, followed by bowel distension. First, examine and restore bladder drainage. If the patient has an indwelling catheter, check for a UTI and make sure it isn't blocked, broken, or in the wrong place.
To assess patency, irrigate the catheter with warm normal saline. Use little watering. If the Foley catheter isn't working, it should be replaced. Overly pushing, tapping, or palpating the bladder may worsen dysreflexia. Immediately install a Foley catheter if the patient doesn't have one.
Before implantation, anesthetic gel should be placed in the urethra for two minutes. Increased sympathetic tone may tighten the urethral sphincter, making it hard for people with autonomic dysreflexia to place a Foley catheter. If Foley installation is problematic, use a coude catheter or guidewire.
Emergency Antihypertensive Treatment
If the triggering event cannot be determined and early measures do not reduce the patient's systolic blood pressure to less than 150 mmHg or less than 40 mmHg over the patient's typical baseline, emergency antihypertensive pharmacologic therapyshould be commenced. Hypertension should be treated as soon as possible with drugs that start working quickly but don't last long.
- Nitroglycerine 2% Paste: 1 to 2-inch dose (applied on the non-hairy chest or elsewhere above the level of spinal damage). The onset of activity is 3 to 5 minutes The action will last 8 hours. 5 inches is the maximum dosage. Dosage of nifedipine is 10 mg. The activity begins in 10 to 20 minutes, peaks in an hour, and may be repeated every 20 to 30 minutes. The action lasts four hours. The maximum daily dosage is 40 mg.
- The sublingual dose of captopril is 25 mg. The activity begins in 20 to 30 minutes and may be repeated in 1 hour if necessary. The action lasts four hours. The highest recommended dosage is 50 mg.
- Clonidine's sublingual dosage is 0.2 mg. 0.1 mg was added after that. As required, every hour. The activity begins in 10 to 20 minutes. 1 hour of peak activity. The action will last 12 hours. The highest effective dosage is 0.8 mg.
The patient's blood pressure should be monitored for at least two hours after receiving emergency hypertensive medication. The need for continuous blood pressure monitoring should not dissuade doctors from utilizing pharmacological medications when required, since uncontrolled high blood pressure mixed with cerebral vasodilation is very hazardous and possibly deadly.
Patients should be told about possible bad side effects of medical treatment, like tachycardia, rebound hypotension, nausea, vomiting, sleepiness, flushing, and cardiac arrhythmias.
People Also Ask
What Triggers Autonomic Dysreflexia?
The most common cause of autonomic dysreflexia is a full bladder. Other possible causes include stones, kinks in urinary catheters, urinary tract infections, fecal impaction, pressure sores, ingrown toenails, fractures, menstruation, hemorrhoids, and invasive procedures.
What Is The Most Common Cause Of Autonomic Dysreflexia In Spinal Cord Injury?
Spinal cord injuries are a leading cause of autonomic dysreflexia. Autonomic dysreflexia is a condition in which the nervous system overreacts to stimuli that would have no effect on a normally functioning person.
What Is The Commonest Precipitant Of Autonomic Dysreflexia In Patients With Spinal Injury?
After a spinal cord injury, autonomic dysreflexia may be triggered by any painful stimulation below the damage site. Most cases of autonomic dysreflexia are caused by stimulation of the lower urinary tract, and in 75% to 85% of these cases, the cause seems to be a full bladder.
Final Words
Autonomic dysreflexia develops after a spinal cord injury and may result in life-threatening hypertension. Suspect autonomic dysreflexia in people with spinal cord injuries above T6, high blood pressure, and increased sympathetic activity, especially if they have hollow viscus distention, which is often caused by a blocked bladder catheter. If feasible, treat severe hypertension with fast-acting medications.

Suleman Shah
Author
Suleman Shah is a researcher and freelance writer. As a researcher, he has worked with MNS University of Agriculture, Multan (Pakistan) and Texas A & M University (USA). He regularly writes science articles and blogs for science news website immersse.com and open access publishers OA Publishing London and Scientific Times. He loves to keep himself updated on scientific developments and convert these developments into everyday language to update the readers about the developments in the scientific era. His primary research focus is Plant sciences, and he contributed to this field by publishing his research in scientific journals and presenting his work at many Conferences.
Shah graduated from the University of Agriculture Faisalabad (Pakistan) and started his professional carrier with Jaffer Agro Services and later with the Agriculture Department of the Government of Pakistan. His research interest compelled and attracted him to proceed with his carrier in Plant sciences research. So, he started his Ph.D. in Soil Science at MNS University of Agriculture Multan (Pakistan). Later, he started working as a visiting scholar with Texas A&M University (USA).
Shah’s experience with big Open Excess publishers like Springers, Frontiers, MDPI, etc., testified to his belief in Open Access as a barrier-removing mechanism between researchers and the readers of their research. Shah believes that Open Access is revolutionizing the publication process and benefitting research in all fields.

Han Ju
Reviewer
Hello! I'm Han Ju, the heart behind World Wide Journals. My life is a unique tapestry woven from the threads of news, spirituality, and science, enriched by melodies from my guitar. Raised amidst tales of the ancient and the arcane, I developed a keen eye for the stories that truly matter. Through my work, I seek to bridge the seen with the unseen, marrying the rigor of science with the depth of spirituality.
Each article at World Wide Journals is a piece of this ongoing quest, blending analysis with personal reflection. Whether exploring quantum frontiers or strumming chords under the stars, my aim is to inspire and provoke thought, inviting you into a world where every discovery is a note in the grand symphony of existence.
Welcome aboard this journey of insight and exploration, where curiosity leads and music guides.
Latest Articles
Popular Articles