Periodontal Tissue Generation Using Autologous Dental Ligament Micro-Grafts [Case Report]
A new clinical process of tissue regeneration has been devised through stem cell research. Here is a study about periodontal tissue generation using autologous dental ligament micro-grafts.
Author:Suleman ShahReviewer:Han JuNov 06, 202410.9K Shares731.6K Views

In the previous years, stem cell research has found several problems in transferring the scientific models into clinical practice, and here is where periodontal tissue generation using autologous dental ligament micro-graftsenters the picture.
Using an autologous micro-graft named Rigenera, the patient is, at the same time, the donor and the acceptor of calibrated micro-graft rich in stem cells.
This system permits an increase in the stem cell number in the surgical site that needs to be regenerated. This case report was performed to analyze the clinical outcomes of an innovative treatment protocol of deep intra-osseous periodontal defects using dental ligament micro-grafts loaded onto collagen sponges as filling biomaterial.
Preliminary Discussion
The increasing research on autologous stem cells and their abilities gave an input to the study of self-regenerative potential of the injured tissues - the presence of autologous cells reservoir able to provide elements to restore the periodontal tissues is extremely intriguing and enforces the concept at the base of conservative and minimally invasive surgery.
The problem of these cell reservoirs is the surgical management, because often we do not have tools and procedures to use them for clinical application.
In this study we present a split-mouth case report, where an autologous dental ligament was used to generate micro-graft through a new technologycalled Rigenera Protocol.
This protocol is made by a machine, the Rigenera Machine, and disposable medical devices, the Rigeneracons (a registered name), able to mechanically break-up small tissue samples, preserving cell viability.
From the 1960s periodontal research has been interested in regenerating the periodontium, moving on a wide spectrum of hypotheses, such as the use of:
- biomaterials
- biomolecules
In the previous years, the approach has pointed to increasing the self-regenerative potentials of the injured tissues, in order to reduce complications and make the results more predictable.
In recent years, it has been supposed to collect stem cells from a rich zone and use these cells to treat diseases or trauma of tissues with a limited self-regenerative potential, thanks to their particular plasticity.
Therapeutic protocols for homologous and autologous human transplantation have been conducted with different results.
Actually, the surgical access to these potential collection sites often is a limiting point, and the ratio between the tissue collected and stem cells isolated is often disadvantageous.
The dental ligament has been shown to own stem and progenitor cells able to restore the periodontium. We used the dental ligament of an extracted impacted wisdom tooth to restore the periodontal defect of another molar of the same patient.
Intraosseous pockets are bony defects of the periodontal complex, occurring as a result of infection of bacteria and exiting in a bone resorption.
After adequate therapy, it is possible to obtain the resolution of the infection but not the restitutio ad integrum (Latin for “restoration to original condition”) of the tissue injured, and these defects can represent niches for a new infection or limit the functional activity of the tooth affected.
The aim of this study was to apply dental ligament micro-graft, rich with progenitor cells, to the tissue engineering for periodontal regeneration.
This approach has never been used before in this field and their success could open new strategies to clinical therapies of the chronic periodontal disease that currently affects up to 40% of the adults in western countries.
Case Report
We performed a split-mouth study.
The patient: MC, female, 32 years old. She had two intraosseous defects distal to the second lower molars due to mesio-impact of both vital third molar included.
The patient was:
- healthy from systemic diseases
- a non-smoker
The hygiene phase of the periodontal therapy included:
- oral hygiene instructions
- supra-gingival and sub-gingival scaling
- root-planning under local anesthesia
- limited occlusal adjustment
The selected teeth presenting the intraosseous defect were vital and had at least a 2-millimeter zone of buccal keratinized gingiva.
The patient had a medical historymaking her qualified for dentoalveolar surgery (i.e., ASA I). The patient had to sign an informed consent form prior to surgery. She agreed to carry out all study procedures and follow all instructions.
To recap, we selected a healthy female patient, with two intraosseous defects.
We used the two defects:
- one as a test site (cell suspension + collagen sponge scaffold)
- the other, as a control site (only collagen sponge scaffold)
Clinical and radiographic examination was performed at baseline and at 1 week and at 1, 3, and 6 month/s after surgery.
The x-rays performed at 3 and 6 months show significant differences between the control site and test site: the latter presented an increased mineralization rate and the complete filling in the coronal component of the defect with respect to the control site.
Surgical Intervention
Prior to the surgery, facial skin was cleaned with 4% Chlorhexidine (CHX). The oral decontamination was obtained using 60 seconds of mouth rinsing (using Forhans medical mouthwash), with 0.2 CHX washing.
The local anesthetic used was articaine (2%), with an epinephrine concentration of 1:100,000 (meaning, 1 gram of epinephrine dissolved in 100,000 milliliters of solvent). Ubistesin is a brand of articaine by 3M ESPE.

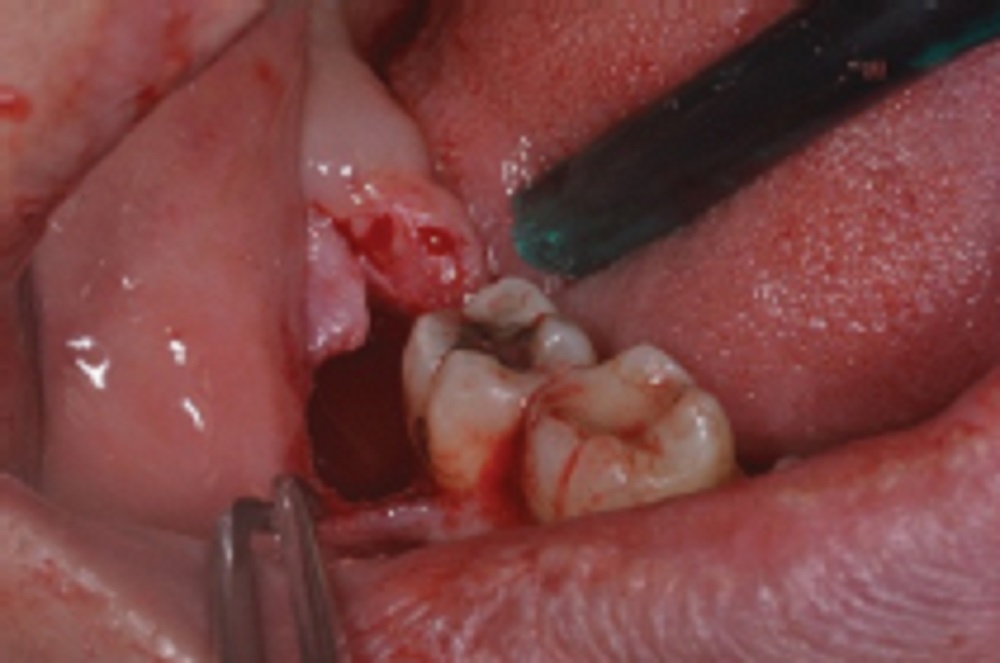
Then the third molar was extracted and cleaned using CHX 0.2 for 60 seconds (see picture above).
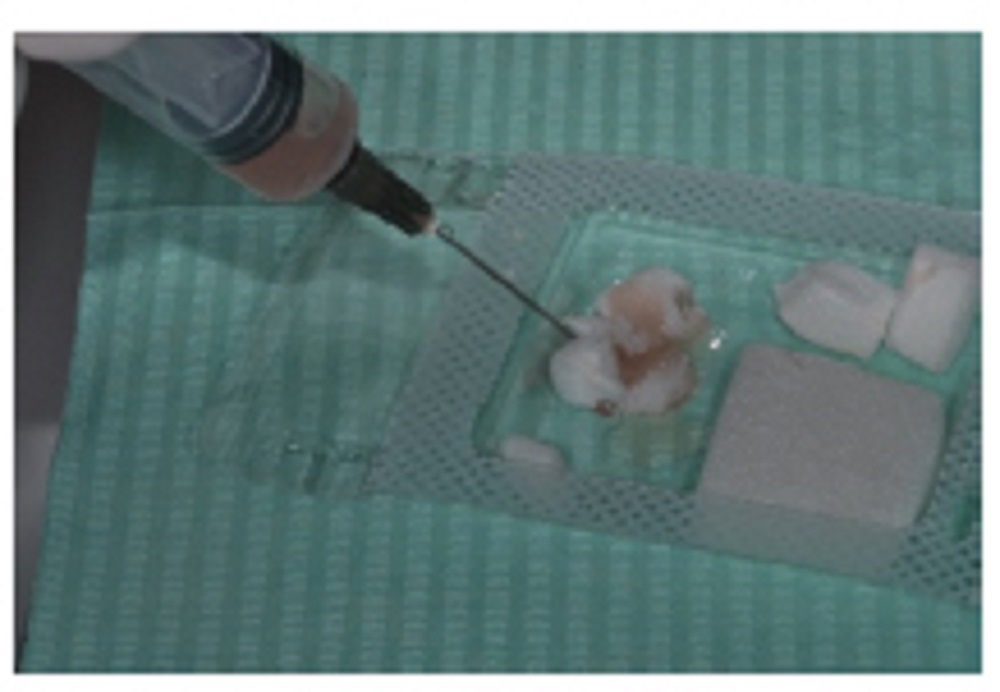
The dental ligament attached to dental roots was gently collected using a Gracey curette and dissociated using Rigenera System with Rigeneracons sterile filters (Rigenera HBW or human brain wave from Turin, Italy) in 2 ml. of sterile physiologic solution (see picture below).

This tool permits the simultaneous mechanical digestion of the dental pulp and the filtering of the solution through a 50-μm strain. After 60 seconds of agitation, the cellular suspension is collected from the system and used to wet a collagen sponge (Gingistat from dental supply store Gaba in Milan, Italy), that has no radiopacity at all (see picture below).
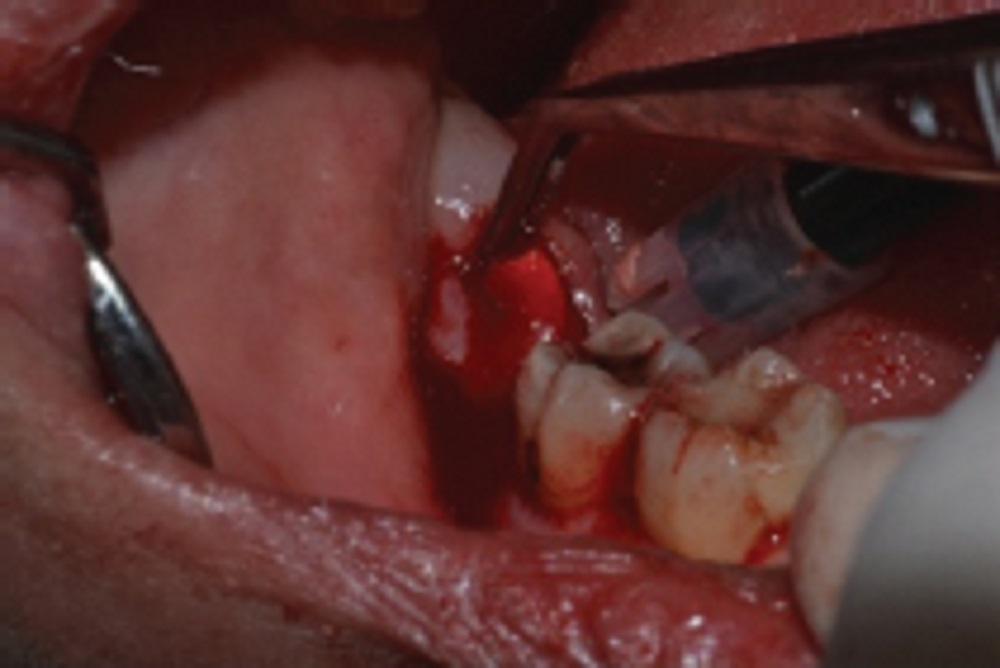
After elevation of the flap, all the inflammatory tissue was removed and the defect walls cleaned with hand and ultrasonic instruments (see picture below). The root of the tooth underwent the same treatment.
In the test site the enriched collagen sponge is gently placed within the intraosseous defect and the suture performed using non-absorbable suture (3-0 Silk; Ethicon, a Johnson & Johnson subsidiary; and Sint-Stevens-Woluwe, Belgium).
In the control site, we used only the collagen sponge.

Post-surgical medications were prescribed as follows:
| Medication | Prescription |
| amoxicillin (875 mg.) + clavulanic acid (125 mg.) | twice a day for 6 days |
| ibuprofen (600 mg.) | twice a day for 5 days |
| 0,12% Chlorhexidine | rinse twice a day for 15 days |
Note:For the said antibiotic therapy, GlaxoSmithKline’s (GSK)Augmentin (amoxicillin and clavulanate) was used. The ibuprofen taken was Brufen by Abbott. The brand of Chlorhexidine (CHX)mouthwash used was Curasept.
Post-surgery, the patient complained of neither swelling nor pain. The post-surgical course was uneventful. The sutures were removed after 7 days.
During the first week after the surgery, the patient was instructed:
- to avoid traction and chewing on the area
- to limit mechanical hygiene on that side of the mouth
House hygiene was obtained only using CHX 0,12% rinses three times a day for 6 weeks. After 4 weeks, the patient was advised to restore chewing and mechanical hygiene in that area using brush and interproximal tools.
All patients were subjected to supra-gingival professional tooth cleaning by means of a rubber cup, with polishing paste at 1, 3, and 6 months after surgery.
Sub-gingival hygiene was never performed.
Clinical Examinations
Clinical examination was performed at baseline and at 1 week and at 1, 3, and 6 month/s after surgery.
Baseline measurements were performed on the day of surgery. All clinical measurements were undertaken by one experienced periodontist.
All the measures of this study were taken by the same calibrated examiner using a PCP UNC15 Perio Probe (it’s a Williams periodontal probe by Hu-Friedy, a Chicago-based medical equipment manufacturer) and approximated to the nearest millimeter (mm.).
Presence or absence of visible dental plaque adjacent to the gingival margin was recorded at the locations of the clinical measurements.
Recorded at the following six sites around each tooth were:
- the presence or absence of marginal or papillary gingivitis
- probing depth (PD)
- clinical attachment level (CAL)
- gingival recession
- bleeding on probing
Height of keratinized gingiva at the three buccal sites was also recorded. Clinical measures were performed at baseline and at 6 months evaluation.
After the first week, clinical controls were scheduled at months 1, 3, and 6.
The patient complained of symptoms neither during the first week nor during the following period after the surgery. The gingiva surrounding the defect was neither found edematous nor ulcerated.
The PD before the surgeries was:
- 12 mm. for the test
- 11 mm. for the control
The surgical CAL was:
- 6 mm. for the test
- 5 mm. for the control
After 6 months, the PD was:
- 3 mm. for the test
- 7 mm. for the control
Radiographic Examination
A dental cone beam computed tomography (CBCT) scan was taken before the surgery - the impacted molars provoked the reabsorption of the alveolar bone process distal to the second lower molars (see picture below).
Standardized periapical radiographs were obtained by a periodontist at 3 and 6 months after periodontal surgery.
At 3 months, both test and control showed immature bone formation. At 6 months, the radiographs (RX) in the test site, the mineralization was higher than in the control site.
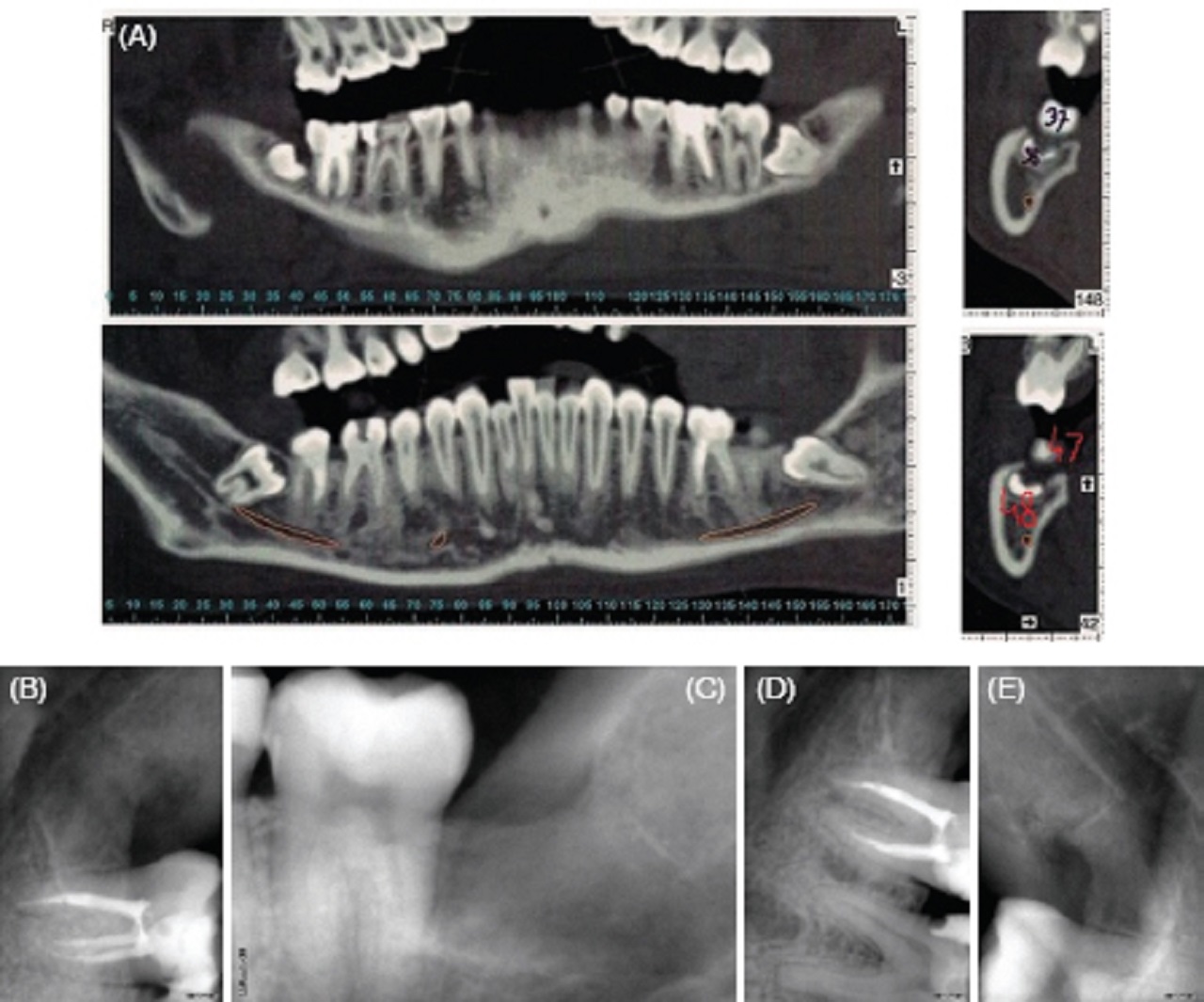
Additional information about the picture:
a. (A) The CBCT before the surgery, no alveolar bone was present distal to the second lower molars.
b. (B) The endoral RX after 3 months of the surgery in the test and (C) in the control site.
c. The endoral RX after 6 months in the test (D) and in the control site (E).
Discussion
This study was performed to analyze the clinical outcomes of an innovative treatment protocol of deep intra-osseous periodontal defects using dental ligament micro-grafts loaded onto collagen sponges as filling biomaterial.
This surgical approach was made possible by the Rigenera System.
In a comparative study published in 2008 by the Journal of Craniofacial Surgery, the authors, with Francesco Carinci as lead author, showed advantages of the use of stem-derived osteoblastsversus the primary cultured osteoblast.
The in vitro and in vivo studies performed in animal models showed that the stem cell fraction was constituted by cells under the 70 μ diameter. Under this cut-off dimension, the percentage of cells expressing stem antigens grows dramatically, avoiding a magnetic or flow cytometry sorting.
The efficacy of this approach of cell selection has been recently demonstrated in clinical protocol to regenerate human mandibular defects.
In this experimental study on 17 patients, the enzymatic digestion of the pulpar tissue was substituted by mechanical digestion, guaranteeing in this way a close flow of the manipulation passages leading to stem cells isolation.
The cell suspension was then used after loading on collagen sponges, and the results after 6 months of follow-up was very encouraging when compared to the control of a non-treated bone defect resulting after impacted third molars extraction.
Although it remains well established that currently available regenerative technologies, such as membranes and EMD (enamel matrix derivative), may lead to a true regeneration of the periodontal tissues lost due to periodontal diseases, we designed our protocol for periodontal regeneration using the dental pulp stem cells, cells that have shown significant bone regeneration activity in clinical protocol.
Also, although bone engineering is the main application field for these cells, their antigenic profile makes them suitable for tissue engineering.
Their behavior in the presence of scaffold has been investigated, and they showed better performance when compared with osteogenic primary culture.
In this study, we investigated the possibility of the dental ligament to regenerate the entire periodontal complex, constituted by:
- ligament
- cementum
- bone
All the periodontal tissues come from progenitor cells that, in origin, come from the neural crest-derived mesenchymal cells.
These cells originate during the embryologic period in the neural crests and then migrate into the cranial region of the embryo, originating from the dental buds and surrounding tissue.
After development, some of these cells remain embedded within the tissues, although in a very low percentage. A niche, where it is possible to isolate these stem cells after the birth, is the dental pulp.
As demonstrated in several papers, this anatomical site is an affordable collection place characterized by low morbidity for the region and the patients itself.
The mechanical digestion of the dental ligament brings to a significant cell amount able to regenerate bone chips.
The same protocol in this study has been used to obtain a cellular suspension to mix with a collagen III scaffold, chosen for its mechanical and biological properties.
At first we needed a scaffold able to sustain cells during their differentiation and to ensure mechanical stability to the coagulum that occurs in the regenerating site. Actually, stability is a key factor for cell differentiation; crucial when the committed tissue is a mineralized tissue like the root cementum or bone.
On the biological side, we chose collagen III sponge because collagen III is the main component of the organic structure of an undifferentiated mesenchymal tissue like the surrounding tissues of the dental buds during embryological period into the jaws.
Wetting the collagen III sponge with the micro-graft suspension after tissue dissociation, we reconstitute an activated undifferentiated tissue, able to produce by itself BMP-2 (bone morphogenetic protein) and VEGF (vascular endothelial growth factor) for vascular net claiming and cell bridging.
Then this cell suspension was grafted in the osseous defect, with a mini-invasive surgical technique to avoid the depletion of the residual regenerating activity of the surrounding tissues that can occur after an extensive surgical trauma.
For the first 3 months, we avoided performing an x-ray, although the emission dose is very low, in order to exclude any x-rays damaging the proliferating cells.
The x-rays performed at 6 and 12 months confirmed the increase of the mineralization rate, probably due to the remodeling of the woven bone into lamellar bone.
Our technique provides a mini-invasive procedure for stem cell application in periodontal surgery acting as a “biotechnological graft” for these types of defects.
Taken together, these data are very encouraging, although a much bigger number of cases must be treated and analyzed to confirm the efficacy of this technique.
Conclusion
The results indicate that the autologous stem cell obtained from connective tissue could be used to provide the basis for bone regenerative surgery, with:
- limited sacrifice of tissue
- low morbidity at the collection site
- significant reduction in time needed for clinical recovery
From the x-ray analysis, the more interesting data are the complete filling in the coronal component of the defect - this pattern of regeneration is more similar to those obtained with membranes than with molecular factors.
The limit of this approach is that it can be used only in selected patients with a hopeless but vital tooth that can act as a donor site of dental ligament.
Nevertheless, this situation is often present in patients with chronic periodontitis, which needs the extraction of the wisdom tooth or other hopeless teeth during osseous resective surgery.
This therapy has never been used before for this purpose, and it seems a very promising tool for the treatment of these defects.
Therefore, more studies should be conducted regarding periodontal tissue generation using autologous dental ligament micro-grafts.

Suleman Shah
Author
Suleman Shah is a researcher and freelance writer. As a researcher, he has worked with MNS University of Agriculture, Multan (Pakistan) and Texas A & M University (USA). He regularly writes science articles and blogs for science news website immersse.com and open access publishers OA Publishing London and Scientific Times. He loves to keep himself updated on scientific developments and convert these developments into everyday language to update the readers about the developments in the scientific era. His primary research focus is Plant sciences, and he contributed to this field by publishing his research in scientific journals and presenting his work at many Conferences.
Shah graduated from the University of Agriculture Faisalabad (Pakistan) and started his professional carrier with Jaffer Agro Services and later with the Agriculture Department of the Government of Pakistan. His research interest compelled and attracted him to proceed with his carrier in Plant sciences research. So, he started his Ph.D. in Soil Science at MNS University of Agriculture Multan (Pakistan). Later, he started working as a visiting scholar with Texas A&M University (USA).
Shah’s experience with big Open Excess publishers like Springers, Frontiers, MDPI, etc., testified to his belief in Open Access as a barrier-removing mechanism between researchers and the readers of their research. Shah believes that Open Access is revolutionizing the publication process and benefitting research in all fields.

Han Ju
Reviewer
Hello! I'm Han Ju, the heart behind World Wide Journals. My life is a unique tapestry woven from the threads of news, spirituality, and science, enriched by melodies from my guitar. Raised amidst tales of the ancient and the arcane, I developed a keen eye for the stories that truly matter. Through my work, I seek to bridge the seen with the unseen, marrying the rigor of science with the depth of spirituality.
Each article at World Wide Journals is a piece of this ongoing quest, blending analysis with personal reflection. Whether exploring quantum frontiers or strumming chords under the stars, my aim is to inspire and provoke thought, inviting you into a world where every discovery is a note in the grand symphony of existence.
Welcome aboard this journey of insight and exploration, where curiosity leads and music guides.
Latest Articles
Popular Articles