Rotator Cuff Tears, Evaluation And Treatment - A Critical Review
Injuries commonly affecting the group of muscles and tendons surrounding the shoulder joint include rotator cuff tears. Treatment can vary depending on the injury’s severity.
Author:Suleman ShahReviewer:Han JuJan 19, 202487 Shares86.8K Views
Rotator cuff tearsare a common cause for shoulder pain in the older population.
The etiology and pathophysiology are not fully understood. Theories for tear evolvement are divided into:
- intrinsic (e.g., recurrent microtrauma)
- extrinsic (e.g., subacromial impingement)
The subacromial bursa is probably the source of pain in symptomatic patients with rotator cuff tears. It is uncertain whether the tear itself can produce pain because of the high prevalence of asymptomatic tears.
Typically, there is a gradual increase in shoulder pain and weakness; however, it can present acutely due to an injury.
Difficulties in overhead activities and night pain are common.
Imaging such as ultrasound and magnetic resonance are required for accurate evaluation of rotator cuff tears in patients with ongoing pain and limitations.
Primary treatment includes:
- activity modifications
- pain relief
- physical therapy
Surgery is advised for acute tears in active patients or chronic symptomatic tears in patients that fail to improve.
This article discusses the evaluation and treatment of rotator cuff tears.
Pain In The Shoulder
Shoulder pain is a very common complaint.
Studies report on about one-third of the population that suffer from shoulder symptoms during their lifetime.
One of the main causes for shoulder pain in the older population is rotator cuff tears. The prevalence of rotator cuff tears in the general population is 20%.
Without appropriate evaluation and treatment, the pain may persist for a long period of time.
Since the early 1990s, there has been a significant progress in arthroscopic surgery techniques for symptomatic tears of the rotator cuff. Currently, selected patients are treated with these techniques with high success and low morbidity rates.
The aim of this review was to discuss the methods for evaluation and the treatment techniques for rotator cuff tears.
Anatomy
There are two synovial spaces in the shoulder:
- glenohumeral space
- subacromial space
Between those spaces is the rotator cuff complex of four tendons together with the underlined joint capsule. These are the:
a. Supraspinatus, Infraspinatus, and Teres Minor
- originate from the posterior scapula
- insert into the greater tuberosity of the proximal humerus
b. Subscapularis
- originate from the anterior scapula
- insert into the lesser tuberosity
The rotator cuff moves and stabilizes the humeral headin the center of the glenoid by the principle of coupling forces.
The subacromial bursa is localized in between the rotator cuff below and the acromion with the coracoacromial ligament (CAL) above.
The normal separation between the glenohumeral and subacromial spaces is violated when there is a full-thickness tear of the rotator cuff.
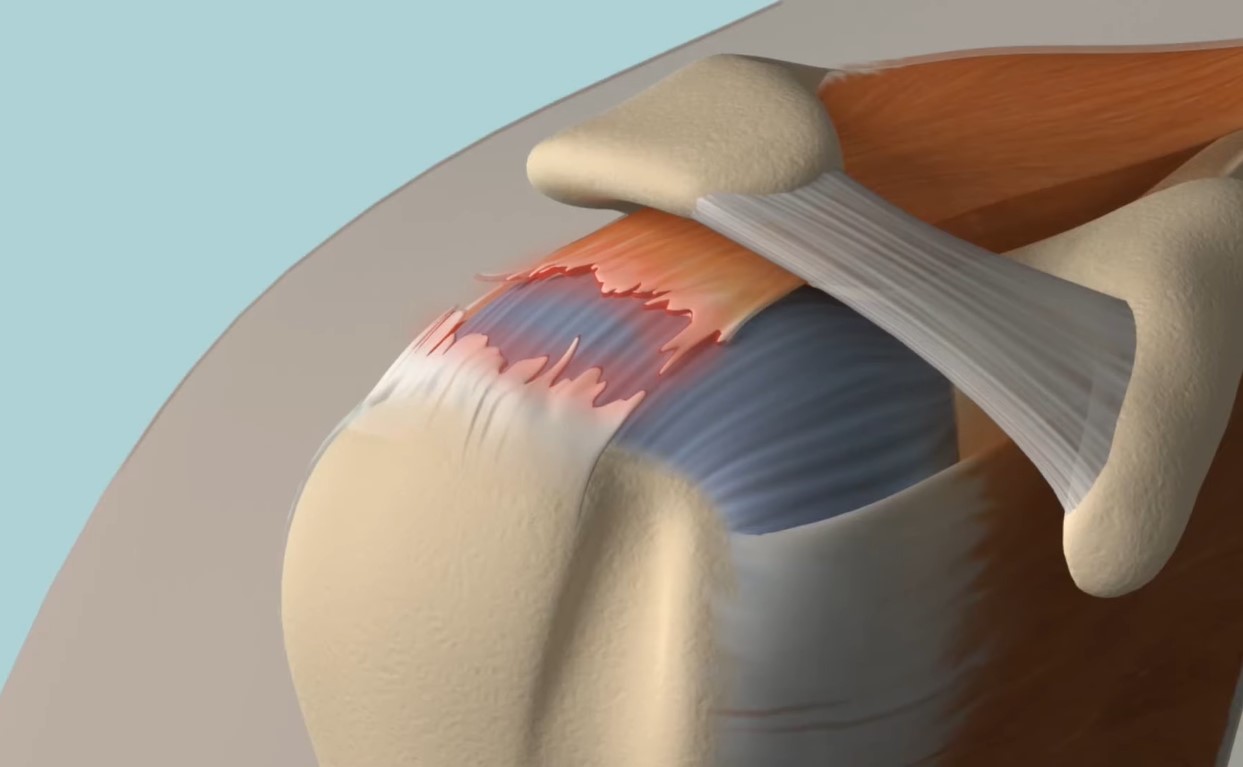
The most common tear of the rotator cuff involves the supraspinatus tendon. This tendon has a unique structure of several parallel independent fiber units that allows for wide-ranging mobility.
During movement, some units are elongated, while othersare shortened. The sheering forces that are produced can cause pathology.
Tear Types
Accurate description of rotator cuff tears is essential for clinical and academic purposes.
Measurements can be done by imaging or at surgery.
It is usually defined by:
- the tendon involved
- its thickness (partial or complete)
- size (anterior to posterior)
Crescent shape tear is the most common full-thickness configuration.
Pathophysiology
In his book The Shoulder: Rupture of the Supraspinatus Tendon and Other Lesions in or about the Subacromial Bursa (1934), American surgeon Ernest Amory Codman (1869-1940) described a hypovascularized zone adjacent to the supraspinatus insertion site.
Although the pathological process is not fully understood, it is degenerative and deteriorates with age. Imaging studies have shown that the prevalence of asymptomatic rotator cuff tears is 30% and 65% in people older than 60 and 70 years, respectively.
Traditionally, the pathophysiological theories are divided into intrinsic and extrinsic.
Intrinsic Tendinopathy
The pathological process involves the tendon tissue.
The main model is degenerative with age-related deterioration into partial-thickness and then full-thickness tendon rupture.
Because of recurrent micro-trauma:
- inflammatory mediators alter the local environment
- oxidative stress causes tenocyte loss with further degeneration
Both histological examinations of tendon tissue and overload animal models have demonstrated changes in blood supply as well as in concentrations of:
- cells
- collagen
- proteoglycans
In addition, studies have shown:
- loss of fibrous organization
- tissue weakening
- high levels of inflammatory markers
Shoulder abduction causes relatively high mechanical stresses in the articular side compared to bursal-sided fibers of the suprasinatus tendon.
These forces produce cartilage tissue near the insertion of the supraspinatus tendon into the greater tuberosity as was demonstrated in other parts of the body. This cartilaginous tissue has weaker load resistance.
In their study published in 1993 by the journal Arthroscopy: The Journal of Arthroscopic and Related Surgery, Stephen S. Burkhart, J. C. Esch, and R. S. Jolson have described the ‘rotator cuff cable,’ a thick crescent-like structure adjunct to humeral insertion site of the rotator cuff.
The cable is perpendicular to the tendon fibers where the medial fibers between it and the humerus are thinner and localized in the hypovascular critical zone described by Codman.
Although the cable has biomechanical advantages derived from the suspension bridge mechanical principle, these medial fibers tend to wear and tear.
The vascular supply to the supraspinatus tendon has been studied for many years.
The common theory suggests a critical hypovascular zone at 10 to 15 millimeters from its insertion site into the humerus.
However, several studies have contradicted this theory.
Thus, the relationship between vascular supply and degeneration is not entirely clear. Nevertheless, the tear margins are often avascular with limited healing potential.
Extrinsic Tendinopathy
The pathological process is external to the tendon tissue.
In his study published in 1983 by the journal Clinical Orthopedics and Related Research, American orthopedic surgeon Dr. Charles S. Neer, II (1917-2011) has suggested the coracoacromial arch as the primary offender.
The recurrent attrition of the tendons against the inferior part of an aberrant acromion causes tissue damage.
According to the authors of a study published in 1991 by the Clinical Journal of Sport Medicineand led by orthopedist Dr. Louis U. Bigliani, there are three morphological types of acromion.
Of these, curved or hooked acromion morphologies are found in most patients with rotator cuff tears.
Based on the above assumptions, one of the most popular surgical techniquesof the shoulder is acromioplasty (resurfacing the lower edge of the acromion), although its correlation with clinical results is currently debatable.
Pain receptors have been found at the CAL, and some authors believe that it may cause external impingement, while others claim that the pathological changes within the CAL are secondary to chronic mechanical tension and do not cause rotator cuff tears.
Surgical detachment of the CAL may cause superior migration of the humeral head, and therefore, it is important to try and preserve it.
Theoretically, subacromial impingement should trigger a partial tear at the subacromial tendon side; however, there are many reports on partial supraspinatus tear at its articular side.
This has led to the internal (or superior posterior) impingement theory in which the rotator cuff is compressed between the posterior glenoid margins and the greater tuberosity.
Several demographic factors have been implied to be correlated with rotator cuff tears.
For example, it would be logical to assume higher tear rates in the dominant shoulder; still, about one-third of the patients with symptomatic tears have asymptomatic contralateral full-thickness tears, and most patients with symptomatic tears are not manual laborers.
Another example is the negative effect of smoking on tendon healing, which was evident after surgical repair and in animal studies.
The Source Of Pain
The source of pain in rotator cuff abnormalities is still unclear.
Ruptured rotator cuff does not cause pain directly since there are many asymptomatic full-thickness tears.
It is generally believed that the subacromial bursa is a major source of pain and discomfort as it undergoes some friction during shoulder movement and has sensory nerve endings.
In addition, the pain level was found to be correlated with the subacromial bursitis.
The bursa is innervated anteriorly by the suprascapular nerve and posteriorly by the lateral pectoral nerve.
It contains nociceptors and proprioceptors. These receptors and the presence of mechanoreceptors under the CAL imply a reflex system that coordinates the rotator cuff maintenance of humeral head position.
Found in patients with shoulder impingement syndrome are high levels of:
- pain-associated proteins (e.g., substance P)
- inflammatory cytokines (e.g., IL1)
- collagen-catabolic proteins
Diagnosis
The rotator cuff may rupture acutely due to trauma, but often the clinical presentation is gradual with progressive pain and weakness around the shoulder.
Pain increases:
- with shoulder elevation
- with internal rotation
- at night
Shoulder strength depends on the tear size and the overall function of other intact tendons.
Physical findings that are suggestive of tear are:
- muscle atrophy
- subacromial tenderness
- crepitation
Strength and motion may be limited depending on the muscle involved.
Massive tears may cause shoulder instability. Thus, when trying to elevate the arm, the humeral head subluxates anteriorly. In this position, the deltoid muscle cannot efficiently abduct the arm.
This clinical presentation is called pseudo-paralysis.
Imaging techniques are required if an acute tear is suspected or whenever the pain does not resolve.
Plain radiographs are recommended as the primary modality to rule out other pathologies such as arthritis and to observe acromial morphology with its distance from the humeral head (decreased in massive tears); however, ultrasound and magnetic resonance imaging (MRI) are used to define rotator cuff tears.
Studies that have compared imaging modalities to arthroscopic findings have found similar accuracy of MRI and ultrasound in detecting rotator cuff tears with:
- sensitivity of 97%
- specificity of 67%
Discussion
Treatment
Despite numerous publications regarding the treatment of rotator cuff tears, the number of high-level, evidence-based studies is scarce.
Many studies are limited because of:
- variations in control groups
- outcome measures
- short follow-ups
- the ability to generalize outcomes of large referral medical centers to peripheral ones
Therefore, treatment is based on:
- clinical experience
- understanding the anatomy
- management of other tendon ruptures in the body, such as those of the hand
Acute Full-Thickness Tears
This should be repaired in up to six weeks from the injury, especially in relatively young and active patients; otherwise, it might retract and atrophy with irreversible changes.
If not repaired early, these tears may be hard to fix with a bad outcome.
Partial Tear
Three important reminders:
1. Many patients improve without surgery.
2. Patients should be treated with exercises and stretches in order to gain range of motion.
3. Unresolved pain may benefit from arthroscopic debridement.
Chronic Full-Thickness Tears
Many patients improve without surgery.
Conservative treatment includes:
- modifying activities
- exercises
- physical therapy
- analgesics
- non-steroidal anti-inflammatory medications
Subacromial steroid injections temporarily relieve pain.
Recurrent injections should be avoided as they may impair tendon tissue, unless surgery is not considered and prior injections have helped.
Persistent pain and dysfunction may improve with surgical repair of the torn tendon.
Factors that are correlated with good outcome after repair are:
- age under 60 years
- traumatic tear
- short duration of symptoms (less than two months)
- no smoking
- good general health
- few injections (less than four)
- primary repair
- stable shoulder with good range of motion
- no muscle atrophy
- single tendon involvement (supraspinatus)
- experienced surgeon
The probability for recurrent tears after repairs increases with larger tears and atrophied tendons. The rehabilitation after surgery depends on the tear size and the quality of the repair.
In many cases, active range of motion is forbidden for six or more weeks while the overall rehabilitation time may last longer than six months.
Surgical Repair
Rotator cuff tendon repair is one of the most common procedures performed in the shoulder.
During the past two decades, the traditional open approach has shifted to mini open and eventually to an all-arthroscopic minimally invasive technique.
Open repairs have had good results but required partial deltoid muscle detachment.
All arthroscopic techniques allow the treatment of concurrent intra-articular pathologies. It requires small incisions, less soft tissue damage, no deltoid impairment and shorter postoperative pain and rehabilitation.
Arthroscopic repairs have good long-term results but also have a steep learning curve.
Many studies have shown better results with non-recurrent (healed) tears after repairs. Therefore, there is much interest and recruitment of resources in order to achieve a successful repair by modifying important factors such as smoking cessation and enriching the biological environment at the tear site.
However, the most dominant factor, according to the literature, is an anatomical stable fixation of the rotator cuff tear.
Currently, an all-arthroscopic technique is utilized to perform anatomical anchoring of the rotator cuff to the proximal humerus.
Common configurations of fixations are single or double rows.
Double-row fixations were found to have biomechanical advantages over single-row fixations; yet, there were no differences in clinical outcomes.
Conclusion
Symptoms of pain and weakness about the shoulder imply rotator cuff tears.
There are typical impingement signs in physical evaluation together with limited range of motion and weakness.
Plain radiographyis required to rule out other pathologies and observe acromion morphology while ultrasound and MRI are used to define the tear and tendon quality before surgical intervention.
The primary treatments involve activity modification, pain relief and exercises for a few months before considering surgical repair followed by prolonged rehabilitation.
Acute repairs are suggested in traumatic tears in relatively young and active patients.
At present, an all-arthroscopic technique is usually used to repair rotator cuff tears with good long-term results.

Suleman Shah
Author
Suleman Shah is a researcher and freelance writer. As a researcher, he has worked with MNS University of Agriculture, Multan (Pakistan) and Texas A & M University (USA). He regularly writes science articles and blogs for science news website immersse.com and open access publishers OA Publishing London and Scientific Times. He loves to keep himself updated on scientific developments and convert these developments into everyday language to update the readers about the developments in the scientific era. His primary research focus is Plant sciences, and he contributed to this field by publishing his research in scientific journals and presenting his work at many Conferences.
Shah graduated from the University of Agriculture Faisalabad (Pakistan) and started his professional carrier with Jaffer Agro Services and later with the Agriculture Department of the Government of Pakistan. His research interest compelled and attracted him to proceed with his carrier in Plant sciences research. So, he started his Ph.D. in Soil Science at MNS University of Agriculture Multan (Pakistan). Later, he started working as a visiting scholar with Texas A&M University (USA).
Shah’s experience with big Open Excess publishers like Springers, Frontiers, MDPI, etc., testified to his belief in Open Access as a barrier-removing mechanism between researchers and the readers of their research. Shah believes that Open Access is revolutionizing the publication process and benefitting research in all fields.

Han Ju
Reviewer
Hello! I'm Han Ju, the heart behind World Wide Journals. My life is a unique tapestry woven from the threads of news, spirituality, and science, enriched by melodies from my guitar. Raised amidst tales of the ancient and the arcane, I developed a keen eye for the stories that truly matter. Through my work, I seek to bridge the seen with the unseen, marrying the rigor of science with the depth of spirituality.
Each article at World Wide Journals is a piece of this ongoing quest, blending analysis with personal reflection. Whether exploring quantum frontiers or strumming chords under the stars, my aim is to inspire and provoke thought, inviting you into a world where every discovery is a note in the grand symphony of existence.
Welcome aboard this journey of insight and exploration, where curiosity leads and music guides.
Latest Articles
Popular Articles